Flu Season Final Toll — and the Policy Fight Ahead
The 2025-26 flu season closed at 174 pediatric deaths (85% unvaccinated). Two weeks of major policy upheaval: a May 29 Executive Order on the childhood vaccine schedule, a new ACIP charter that still leaves the committee paralyzed under a March court stay, 29 states going their own way, and the FDA setting June 18 as the VRBPAC hearing date for Moderna's mRNA flu shot — with an August 5 approval deadline that could put it on pharmacy shelves this fall. Five actions to take now.

This digest covers two weeks — May 18 through June 1, 2026 — because a technical outage skipped last week's run. A lot happened. The flu season formally ended, a White House executive order reshuffled which childhood vaccines the federal government will actively recommend, and the FDA set a date to evaluate the first mRNA flu shot. Rather than recap everything, this issue focuses on the developments that actually change a decision you might make.
The flu season closed — the numbers and what they mean
The 2025–26 flu season is officially over. CDC's Week 20 FluView report (covering the week ending May 23) declared itself "the final full FluView report of the 2025–2026 season." 1 National influenza-like illness visits fell to 1.6% of outpatient care — below the 3.1% national baseline for the 10th consecutive week, with all 55 reporting jurisdictions at minimal activity.
The season's pediatric death toll finished at 174 confirmed influenza-associated deaths in children. 1 Among children whose vaccination status was known, CDC reported that approximately 85% of those who died had not been fully vaccinated. 2 The full-season burden: an estimated 32 million illnesses, 390,000 hospitalizations, and 24,000 deaths. 1
The season's vaccine delivered only 36% overall effectiveness (95% CI: 33–39%), down from 56% the prior season. 3 The gap is explained by H3N2: the dominant subclade — J.2.4.1 (subclade K) — drifted enough from the vaccine strain that only 1.3% of circulating H3N2 viruses were well-recognized by the antibodies the vaccine was designed to produce. 3 Effectiveness against influenza B was much better — 63–71% depending on age group — which explains why late-season B/Victoria activity caused less damage than H3N2 did earlier.
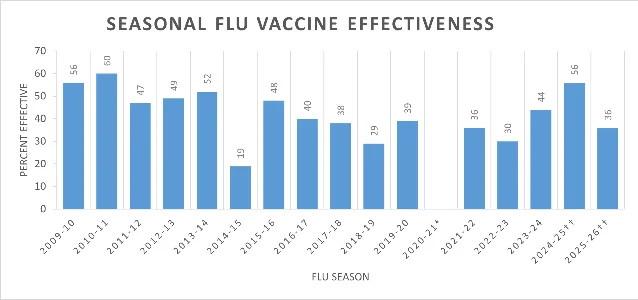
What this means for your family: The 85% unvaccinated fraction in pediatric deaths is the most important number in this report. A shot with 36% overall effectiveness still prevented a substantial share of deaths — imperfect protection at scale saves lives. CDC transitions to streamlined weekly updates through October; the next full surveillance season begins Week 40 (October 4–10, 2026). Start thinking about fall flu shots in August.
The policy earthquake: executive order, charter rewrite, ACIP still paralyzed
The biggest story of this two-week window isn't a virus — it's what happened to the bodies that recommend and govern vaccines.
May 29: Executive order on the childhood schedule
President Trump signed an executive order on May 29 directing the CDC and ACIP to align childhood vaccine recommendations with an HHS scientific assessment that recommends reducing the U.S. core childhood vaccine list from coverage of 17 diseases to 11. 4 Per the White House fact sheet, flu and COVID-19 are among the vaccines the HHS assessment places outside the proposed "core" list. 5
The order explicitly preserves insurance coverage without cost-sharing for all vaccines currently available — it does not ban any vaccine or remove coverage retroactively. 4 What it does is direct ACIP to update its formal recommendations. That's where the problem is: ACIP cannot currently act.
ACIP: new charter, same paralysis
HHS Secretary Robert F. Kennedy Jr. signed a new ACIP charter on May 14, and HHS published a Federal Register notice withdrawing the April charter and re-establishing the committee under the new version on May 19. 6 The new charter removes specific expertise requirements for toxicology, data science, and health economics that the April version had added. It also removes explicit mention of mRNA vaccines as a safety review focus. 7
But none of this restores ACIP's ability to act. A federal court's March 16 preliminary injunction remains in force — it bars 13 of 15 of Kennedy's ACIP appointees from serving and prevents the committee from taking binding action. The June 24–26 ACIP meeting is listed on CDC's website, but the committee cannot vote under the current court stay. 8
Kevin Ault, a former ACIP member who served from 2018–2022, summarized the situation for Healio: "Right now, we don't have a functional way to make vaccine policy without a CDC director." 9 The CDC director seat is currently filled by NIH Director Jay Bhattacharya in an acting capacity; nominee Erica Schwartz has not yet had a Senate confirmation hearing.
Why ACIP's paralysis affects your family directly
ACIP votes trigger two practical consequences: they determine which vaccines insurers must cover at zero cost-sharing under a provision of the Affordable Care Act (ACA Section 2713), and they determine which vaccines pharmacists in most states are legally authorized to administer. No vote = potential coverage gaps and access friction in the fall. 8
The HHS appeal of the March 16 injunction is proceeding slowly — HHS filed its notice to the First Circuit on April 29, more than 7 weeks after the ruling, and no hearing date has been set. 8
States are going their own way
At least 29 states plus Washington, D.C. have taken steps to bypass new federal vaccine guidance. 8 Colorado went furthest: Governor Jared Polis signed SB26-032 in March, letting state health officials follow the recommendations of national medical groups — not just CDC/ACIP — for vaccine purchasing and policy. Colorado state Sen. Kyle Mullica put it simply: "We are insulating our state from the dysfunction coming out of Washington. We're going to rely on science." 10
Iowa moved in the opposite direction: Governor Kim Reynolds signed SF 304 on May 19 limiting teenagers from receiving HPV or hepatitis B vaccines without parental permission, effective July 1. 8 Illinois has a pending bill (SB 3487, passed the state House) that would require hospitals to proactively identify and offer influenza and pneumococcal vaccines to eligible patients per ACIP and state health director guidance. 8
Meanwhile, 2026 measles cases hit 1,952 confirmed cases across 39 states as of May 21 — the Utah-Arizona border remains the largest active outbreak, with Utah reporting 474 cases since January. 11 Measles requires roughly 95% community vaccination coverage to prevent spread; the current vaccine access uncertainty makes maintaining that threshold harder.
What this means for your family:
- The pre-June 2025 childhood immunization schedule remains in force by court order. The American Academy of Pediatrics schedule is the operative clinical reference for pediatricians. Follow it.
- If you're in a state that has codified independent vaccine policy (Colorado, several others), your access is more insulated. If you're in a state that has not, call your insurer's member services now to confirm coverage status for fall flu and COVID vaccines before the September window opens — don't assume the same zero-cost access applies automatically.
- If you have a teenager in Iowa: the parental-consent requirement for HPV and hepatitis B takes effect July 1.
Moderna's mRNA flu shot has a June 18 hearing — here's the timeline
The most significant near-term vaccine news for adults 50 and older: the FDA officially scheduled a Vaccines and Related Biological Products Advisory Committee (VRBPAC) public meeting for June 18, 2026, to evaluate Moderna's MFLUSIVA — that's the commercial name for mRNA-1010, the mRNA-based seasonal flu vaccine. 12 The indication being reviewed: prevention of flu in adults 50 and older. The FDA's formal review deadline (PDUFA date) is August 5, 2026. 13
The underlying data, published earlier in NEJM from a 40,000+ patient Phase 3 trial: mRNA-1010 showed 26.6% better relative effectiveness (95% CI: 16.7–35.4%) against lab-confirmed flu compared to standard-dose vaccine in adults 50 and older. 13 Among adults 65 and older the relative advantage was similar at 27.4%. The comparison was against standard-dose vaccines only — not against the high-dose Fluzone or adjuvanted Fluad that are already preferred for the 65+ group.
Side effects were more common with mRNA-1010: arm soreness (65.8% vs. 29.8%), fatigue (45.1% vs. 20.3%), headache (37.8% vs. 18.0%), and muscle aches (35.4% vs. 11.6%). Most were mild to moderate and short-lived. Serious adverse events were 2.2% vs. 1.9%. 13
One real uncertainty: the FDA advisory infrastructure is not at full strength. FDA Commissioner Makary resigned May 12; Acting Commissioner Kyle Diamantas has been in the role for three weeks as of this writing. 8 The VRBPAC chair stepped down ahead of the June 18 meeting; Iowa University's Stanley Perlman is serving as acting chair. 14 On May 28, a different VRBPAC meeting voted 8-0 (1 abstention) to recommend updating the 2026-27 COVID vaccine to target the XFG subvariant — a normal process that suggests the committee is still functioning on scientific questions even if leadership is in flux. 15
Pfizer's mRNA flu vaccine (PF-07252220) remains in Phase 2 with no data readout announced since February 2026. 16 If the FDA approves Moderna's shot on schedule in August, Pfizer's path to market would realistically be 2027 at the earliest — though Pfizer has not publicly commented on a timeline.
What this means for adults 50+:
- If the June 18 VRBPAC vote is favorable and the FDA acts by August 5, mRNA-1010 could be on pharmacy shelves in time for fall 2026 — but expect limited supply in the first season. High-demand sites may run out early.
- Adults 65 and older who get standard-dose flu shots: you already have better options available right now. Fluzone High-Dose (4x antigen dose) and Fluad (with adjuvant) are ACIP-preferred for your age group and available at most pharmacies today. Don't wait for mRNA-1010 if you're in this group — get one of the enhanced options this fall.
- Adults 50–64 who get standard-dose shots: the mRNA data makes a case for asking about high-dose or adjuvanted options this fall even before mRNA-1010 is available.
Three research findings worth knowing
Maternal flu vaccination is the only protection available for infants under 6 months
A matched cohort study of 147,907 mother-infant pairs in New South Wales, Australia (2016–2019) found that flu vaccination during pregnancy provided 21% protection (95% CI: 10–31%) against the infant being hospitalized or reported with flu in the first 6 months of life. 17 No flu vaccine is licensed for infants under 6 months — maternal vaccination is the only route to any protection for this group. The effect is real but modest; the authors noted that flu hospitalization rates peak in the first 6 months of life, making even a 21% reduction meaningful for a vulnerable age group.
If it has been more than 9 months since your young child's flu shot, the protection may be largely gone
A study tracking 196,593 children under 5 in Singapore found that overall flu vaccine effectiveness was 53% — but by 39–52 weeks post-vaccination, relative effectiveness had waned to just 11–21% of the original level. 18 This is a tropical setting where flu circulates year-round, so direct US comparison is imperfect. But for US families: a shot given in September 2025 may offer reduced protection by May or June 2026, which is partly why timing your annual flu shot in September–October (rather than August) tends to deliver better protection through peak US flu season (typically November–February).
The H3N2 mismatch this season has a specific molecular cause — and recombinant vaccines handled it better
A study published in the Journal of Virology explains at the molecular level why H3N2 effectiveness was so low this year. Egg-grown flu vaccines — which account for most US production — acquire a specific amino acid change (K142R) during the manufacturing process. This reversion reduced the antibody response against the drifted H3N2 strains circulating this season. Recipients of recombinant protein vaccines (specifically Flublok) showed better antibody responses against the same strains. 19 The authors cautioned that this "could impact vaccine effectiveness" — which is exactly what the 2025–26 season demonstrated.
For families who had a choice between egg-grown and recombinant vaccines this season and picked egg-grown: this is the science behind why the season worked out the way it did. Looking ahead to 2026–27, if H3N2 remains dominant and recombinant options are available, that distinction may matter again.
What to do right now
- Review your child's immunization record against the pre-June 2025 AAP schedule. The court injunction keeps that schedule legally in force. Summer camps and fall school enrollment both require up-to-date records — check before August.
- If you have a newborn or are pregnant: get your flu shot now (if you haven't this season) or plan it for early fall. It's the only available protection for babies under 6 months during the first half of next flu season.
- Adults 65 and older: ask specifically for Fluzone High-Dose or Fluad this fall — don't accept standard-dose unless those options aren't available. Both already have ACIP recommendations for your age group. mRNA-1010 may join them; check after August 5.
- Check your insurer's vaccine coverage terms before September. With ACIP non-functional, there is genuine uncertainty about whether the automatic zero-cost coverage trigger (ACA Section 2713) will fire normally for fall flu and COVID vaccines. A quick call to member services now avoids a surprise bill in October.
- If you're in Iowa and have a teenager who needs HPV or hepatitis B vaccine, act before July 1 — that's when the new parental-consent requirement takes effect and the access pathway changes.
Flu surveillance data from CDC FluView Weeks 19 and 20 (ending May 16 and May 23, 2026). Vaccine effectiveness estimates from CDC MMWR, published March 12, 2026; no updated estimates were released in this two-week window. Policy reporting primarily from CIDRAP/Unbiased Science (May 28), Reuters (May 19), Healio (May 22), and White House official releases (May 29). mRNA-1010 clinical data from Moderna/BioSpace citing the NEJM publication. Research findings from peer-reviewed publications indexed on PubMed.
AI-generated cover image.
参考ソース
- 1CDC FluView Week 20, ending May 23 2026
- 2CDC FluView Week 19, ending May 16 2026
- 3CDC MMWR: Interim VE Estimates 2025-26
- 4White House: EO on Childhood Vaccine Recommendations, May 29 2026
- 5White House Fact Sheet: Childhood Vaccine Recommendations, May 29 2026
- 6Federal Register: ACIP Charter Re-Establishment, May 19 2026
- 7Reuters: Kennedy backs away from ACIP charter changes, May 19 2026
- 8CIDRAP/Unbiased Science: State of US Vaccine Policy, May 28 2026
- 9Healio: HHS rolls back ACIP charter changes, May 22 2026
- 10Clinical Advisor: Colorado charts its own course on vaccines, May 2026
- 11Immunize.org IZ Express Issue 1875
- 12FDA VRBPAC June 18 2026 Meeting Announcement
- 13BioSpace: Moderna NEJM Phase 3 mRNA-1010 publication
- 14POLITICO Prescription Pulse: FDA panel to consider Covid shot update, May 27 2026
- 15PharmExec: VRBPAC votes on 2026-27 COVID vaccine, May 28 2026
- 16Pfizer Q1 2026 Pipeline Update, May 5 2026
- 17Pediatric Infectious Disease Journal: Maternal flu vaccine VE in infants
- 18Journal of Infection: Flu vaccine waning in children under 5, Singapore
- 19Journal of Virology: Egg vs. recombinant vaccine strain-specific differences
このコンテンツについて、さらに観点や背景を補足しましょう。